Meeting Children Where They Are: The Neurosequential Model of Therapeutics
Adoption Advocate No. 160
In this practical introductory guide to Dr. Bruce Perry’s Neurosequential Model of Therapeutics, learn how adoptive parents and professionals can implement the wisdom of the NMT, particularly The Sequence of Engagement and the 6 R’s, by using practical neuroscience to guide their everyday work with and care for children and youth who have experienced trauma.
As an adoptive mom and child welfare professional, I have seen firsthand the incredible power of Dr. Bruce Perry’s groundbreaking insight into trauma treatment. On a stifling hot June afternoon, I cradled my 11-year-old son in the backseat of the car, rhythmically patting his back and rocking him after he asked to take a break from a birthday party at the video arcade. Years ago, the party would have ended after a loud, frightening, and embarrassing meltdown, but this day, he placed his hand on his chest and consciously slowed his breathing; I continued to rock in a strong, steady rhythm. Watching the tears roll slowly down his face, I noticed his body start to calm and relax, and after a time, he looked into my eyes and said, “I’m sorry, Mom, it was hot and so loud in there, and the other kids were all getting so many tickets. I felt jealous in my tummy.” He continued to take measured breaths, sat up, and began to play with the squishy fidget in his pocket. He waved out the window to his friends as they streamed out of the arcade to head home. Yes, I knew my boy was far more challenged than his friends by big emotions and transitions. I knew that most 11-year-olds could cope with and even enjoy the flashing lights, noise, and excitement of a day at the arcade, but after years of struggling to change his behavior through sticker charts, consequences, and lectures, this was a huge victory. These 12 minutes of my son's life were the convergence of cutting-edge neuroscience and years of research in the areas of attachment, child development, and trauma. This was the Neurosequential Model in action. This was healing.
What Is the Neurosequential Model?
Bruce Perry, M.D., Ph.D., often begins presentations on the Neurosequential Model of Therapeutics (NMT), with this quote attributed to statistician George Box: “Essentially all models are wrong, but some are useful.” Reminding his audience that no single theory can ever fully capture the unique complexity of a child’s trauma experience is more than just self-deprecating humor. Perry, a psychologist, neuroscientist, and developer of the NMT, designed this model to meet the complex and often challenging needs of children who have experienced trauma. The NMT is not a specific treatment but a way of understanding how both trauma and relationships impact a child’s developing body and brain, and a framework for choosing developmentally effective therapies. Perry and his colleagues have expanded this innovative way of thinking into schools, creating the Neurosequential Model in Education (NME), parenting through the development of the Neurosequential Model of Caregiving (NMC), and coaching with the Neurosequential Model in Sport (NMS). For the many therapists, teachers, and families parenting kids with trauma histories, including my own, the Neurosequential Model has not just been useful—it has been life-changing and vital to the growth and wellbeing of their clients, students, and children.
The NMT approach is based on neuroscience. The brain's core neural networks develop in early childhood. This means what happens prenatally and in the earliest weeks, months, and years of life have long-lasting impacts on the brain and body. Perry writes, "Because the majority of brain growth and development takes place during these first years, early developmental trauma and neglect have a 'disproportionate influence on brain organization and later brain functioning'."[1] The brain develops from the bottom up. The lower areas of the brain mediate the more primitive body-based functions such as heart rate, blood pressure, and respiration, while the higher levels of the brain are responsible for more intricate functions like logic, insight, and reason. When children are exposed to substances or high levels of maternal stress in utero, or to trauma, neglect, and maltreatment early in life, the low brain is often compromised, resulting in unhealthy, inefficient and dysregulated brain function and challenges with higher-brain functions, like relationships and cognition.
Assessment of the functional strengths and deficits of the child is accomplished through the NMT Metric, or Brain Map. Using information about the child’s history of adversity, their current and past relational supports, and measures of development in 32 areas of the brain, the Brain Map provides a snapshot of the child’s current brain-based functioning, their relational health, and their Cortical Modulation Ratio (CRM), an approximate measure of the child’s developmental age. Four critical areas of brain functioning are also scored on the NMT metric: sensory integration, self-regulation, relational function, and cognition.[2] Because these brain regions develop in a particular order (from the bottom up), interventions must also occur from the bottom up. Scores in these areas allow NMT practitioners to select therapies that address the child’s neuro-developmental needs. For example, kids with highly dysregulated sensory integration systems need treatments that create rich sensory experiences and will not receive maximum benefit from interventions such as traditional talk therapies that target the brain's cognitive regions. The Brain Map guides the NMT practitioner in choosing the right intervention at the right time and helps caregivers and other professionals recognize how trauma impacts the child's development, making it much easier to reframe and understand challenging behaviors.
By implementing the wisdom of the NMT, particularly The Sequence of Engagement and the 6 R’s, caregivers and clinicians can use practical neuroscience to guide their everyday work with traumatized kids.
The Sequence of Engagement
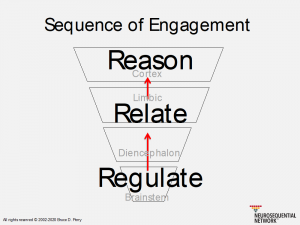 Perry’s Sequence of Engagement is guided by the understanding that when the lower brain is not regulated, well-organized, and efficient the higher brain regions such as the cortex cannot function optimally. When kids are dysregulated or upset, they have little access to the cortex's logic, insight, and reason. Youth with complex trauma histories often struggle with poor behaviors related to low-brain dysregulation, particularly in the areas of sensory integration and self-regulation. In traumatized kids, over-reactions to sounds and touch, hyperactivity, or an inability to smoothly change activities and make transitions are all common behaviors. The NMT helps us recognize these behaviors for what they are: the result of the child’s low-brain dysregulation and sensitized stress response system. Unfortunately, when children are in distress and even in full-on meltdown mode, most parents, teachers, and even therapists are trained to view these behaviors as deliberate choices and respond with “top-down” cognitive approaches. These techniques put us squarely against the brain’s natural survival functions, and more importantly, they just do not work. No amount of talking, reasoning, or reminding a child of the rules ends a meltdown. Until the child is regulated, they cannot reason.
Perry’s Sequence of Engagement is guided by the understanding that when the lower brain is not regulated, well-organized, and efficient the higher brain regions such as the cortex cannot function optimally. When kids are dysregulated or upset, they have little access to the cortex's logic, insight, and reason. Youth with complex trauma histories often struggle with poor behaviors related to low-brain dysregulation, particularly in the areas of sensory integration and self-regulation. In traumatized kids, over-reactions to sounds and touch, hyperactivity, or an inability to smoothly change activities and make transitions are all common behaviors. The NMT helps us recognize these behaviors for what they are: the result of the child’s low-brain dysregulation and sensitized stress response system. Unfortunately, when children are in distress and even in full-on meltdown mode, most parents, teachers, and even therapists are trained to view these behaviors as deliberate choices and respond with “top-down” cognitive approaches. These techniques put us squarely against the brain’s natural survival functions, and more importantly, they just do not work. No amount of talking, reasoning, or reminding a child of the rules ends a meltdown. Until the child is regulated, they cannot reason.
When my son was a preschooler, he had a particularly ugly meltdown in the grocery store. As he lay kicking and screaming in the cereal aisle, I used every parenting technique I had been taught. I redirected, ignored, counted to 10, calmly explained the consequences of his actions, firmly explained the consequences of his actions, then angrily told him he was making me sad and that I was very, very disappointed in him. Nothing worked. I finally picked him up, and we left the store. The next day as I described the situation to his therapist, complaining that my 4-year-old child with a history of neglect and food insecurity, "Just didn't respond to reason," the gentle and wise clinician placed her hand on top of mine and replied, “Yes, that’s true, but remember, you can’t teach a drowning child how to swim.” She explained that what I saw as a defiant meltdown after being told no to sugary cereal in the grocery store was my son's sensitized stress response system reacting to the fear of not getting his needs met. My lectures, well-thought-out explanations, and attempts to convince him through the threat of consequences would never work. To have full access to the logical, rational parts of the brain, the low brain must be regulated.
When we use the NMT as our guide, we focus foremost on regulation through the body and the senses. Engaging with kids through sensory activities like snuggling under a weighted blanket or swinging in a hammock or through movement such as taking a walk or jumping on a trampoline is vital to regulation. Patting my son's back in a slow yet steady rhythm, removing the sensory stimuli of the bright and noisy arcade—these regulate him. Lecturing him about the consequences of his “bad choices” and asking him to reflect on how his behavior impacted me in the grocery store only escalated him.
First, we regulate, then we relate. Relationships are vital in creating a sense of safety and security in children with trauma histories. Adult regulation in the face of the child’s distress and misbehavior is critical. It is easy to become frustrated, irritated, and angry with youth who appear defiant and non-compliant. Yet, it is imperative for adults to maintain a calm, regulated presence in these moments. An angry expression, loud voice, or threatening body posture do not create a sense of safety or positive behavioral change but will typically increase the child’s fear and agitation, leading to even more escalation.[3] Building co-regulation, a state where the adult’s calm, caring presence helps soothe the child, is integral to healing interactions with traumatized kids.
It is only after regulation and relationship that we can begin to reason. This means kids (and adults) must be calm, regulated, and feel safe before they can start the process of learning from or reflecting on their behavior. Only when the child is in this state can they think about what they did, attempt to understand why they did it, repair the mistakes, and reflect on how to avoid these situations in the future. In the reason state, the child can think and talk about what happened, noticing—like my son at the arcade—how emotions, sensations, or the environment may have played a role in their behavior. It took a lot of time to build a strong, healthy relationship and a great deal of commitment to finding the most effective regulation techniques for my son, but his healing, growth, and tenacity were apparent that June day, as The Sequence of Engagement unfolded in real time.
Dr. Perry’s 6 R’s
The 6 R’s are a framework for creating the rich developmental experiences needed to heal trauma. Deeply weaving these tenants into our teaching, treatment, and parenting gives us the decision-making tools to support and strengthen development and mitigate adverse experiences.
1. Relational (safe)
The importance of relationships in healing early trauma and broken attachments cannot be overstated. It is only in the context of relationships that a child’s most critical developmental skills are learned. This is readily apparent when we think about how children learn language. It is only through the relational interaction of a parent talking to them or hearing conversation between adults that infants learn how to speak. Children with histories of maltreatment, neglect, chaotic caregiving, or broken attachments often struggle to feel safe, trust others, or participate in healthy relationships.[4] Because of this, it is critical for adults who care for and work with traumatized children to prioritize relationships. Only when children feel safe and connected can they can learn new skills, grow, and heal.
Tips for building strong relationships:
- We all long to be seen, heard, and understood. Even when kids are misbehaving or dysregulated, adults can engage with empathy, validating their feelings and assuring them that they are not alone in their distress.
- Approach challenging behavior with curiosity, not judgment. Asking a child how you can help or what they need gives us valuable insight into their behavior. Judging behaviors often leads us to assumptions about the child’s motivations or character.
- Be aware of your facial expressions and tone of voice. Children who have been abused and neglected often perceive neutral faces as angry and demonstrate poor recognition of the meaning of facial expressions overall.[5]
- While traumatized kids crave relationships, the intensity of emotional closeness can often be overwhelming or triggering, causing them to shut down or even lash out. When seeking relational opportunities with youth, adults should allow them to have as much control as possible. While we often think connection means looking each other in the eye and sharing our most profound truths, this kind of interaction can be incredibly overwhelming for children with attachment challenges or trust issues. Being side by side, sharing an experience, or completing activities in the same space, and offering, not forcing, interaction, can break down the barriers that children who have lived with trauma and neglect have built to protect themselves.
2. Relevant (developmentally matched to the individual)
Adversity and trauma cause children to have lagging skills in multiple developmental realms; for this reason, we must meet kids where they are. While it sounds simple, this is often incredibly frustrating for parents and professionals who feel children should perform at their chronological age level rather than their developmental age. Carefully observing, reflecting on, and recognizing a child's strengths and weaknesses helps adults have reasonable expectations and know the right times to challenge a child and stretch their skills. In his book What Happened to You? Conversations on Trauma, Resilience, and Healing, co-written with Oprah Winfrey, Dr. Perry states, "It really is never too late. Healing is possible. The key is knowing where to start the process. And matching the developmental needs of the person."[6]
Tips for creating developmentally relevant interactions
- Invest in a new way of thinking. When adults see misbehaviors as lagging skills, they are more apt to respond with kindness and support rather than anger and punishment. Parents, educators, and clinicians must focus their interventions on teaching and strengthening skills rather than shaming kids for their mistakes.
- Have flexible expectations. Remember that stress makes it more challenging to learn and perform. Drop rigid expectations and increase support, especially when children are in new environments, making transitions or among overwhelming sensory stimuli.
- Take note of your child’s lagging skills and strategize about what they might need for support. If you know that loud or chaotic environments or events with lots of relational expectations lead to meltdowns and misbehavior, make sure to plan carefully. Packing a go-bag of sensory tools like fidgets, noise-canceling headphones, crunchy snacks, and chewing gum; remembering to take plenty of breaks during challenging activities; and planning for a quick exit if things get rough can be lifesaving.
3. Repetitive (patterned)
Repetition is essential for creating changes in the brain. This neuroscientific principle is often expressed by the phrase, “neurons that fire together, wire together.” Patterned, repetitive experiences are the basis of all therapeutic and educational growth. Caring adults must provide many opportunities for kids to strengthen their skills and experience safe and healthy relationships. Repetition creates strong neural associations, so the more developmentally rich experiences we can create for our kids, the stronger and more resilient their brains become.
Tips for incorporating repetition:
- Make the child’s life predictable. Routines and consistency create safety and regulation. Have daily schedules, let your child know what's coming next, and provide structured activities that are not overly rigid but feel consistent and supportive.
- Repeat expectations often, even in situations that are common or familiar. For example, while parking the car before having dinner at a restaurant, remind children that they will need to remain in their seats and chat with the family, color or draw, or that they may ask you to take them for a walk while waiting for the food.
- Create multiple opportunities for youth to engage in positive relational interactions. Promoting healthy connections with teachers, coaches, community, and family members allows kids to create new beliefs about themselves, others, and the world. Relationships re-wire the brain.
4. Rewarding (pleasurable)
The human brain is highly motivated by pleasure. We all understand that if an activity or relationship feels good, we want to do it. If it does not feel good, we are not likely to seek it out or may even actively avoid it. When children receive an intrinsic reward, they will typically return to the activity or relationship over and over, without the adult even prompting them. Reward leads to repetition!
Tips for creating rewarding developmental experiences:
- Set aside time for play. Play performs multiple essential roles in child development. It strengthens the imagination; allows children to explore relationships and learn social skills; and helps with problem-solving and physical development. For kids recovering from maltreatment, play can be a way to express big emotions and fears and a safe means to connect with adults. Think of play-time as a way to build your child's skills, form or deepen relationships, and stimulate growth after trauma. Simply adding five minutes of child-directed play to your daily to-do list can develop your child’s confidence, relationships, and resilience.
- Use children’s interests and preferences to provide opportunities for learning and connection.
5. Rhythmic (resonant with neural patterns)
In a 2018 interview, Dr. Perry said, “One of the most destructive effects of trauma is when the stress response systems of the brain become dysregulated...patterned, rhythmic, repetitive activity can restore regulatory balance.”[7] Patterned, repetitive activities get the body ready to learn by balancing and organizing the low brain. Remember, rhythm regulates.
Tips for incorporating rhythm in your interactions:
- One of the most common rhythmic regulation techniques is rocking and singing to an infant. While you may not rock an 11-year-old, you can listen to or make music with him. Creating calming playlists for your home, classroom, or office (songs with 60-80 beats per minute are recommended as they mimic the rate of the human heartbeat); choosing a transition song to play when shifting activities; or working together to create a chant, poem, or rap are some doable and straightforward examples of rhythm at work.
- Playing handclapping games or reciting poetry and nursery rhymes are great ways to spend long car rides or time waiting in lines.
- Do not wait until kids are dysregulated. Be proactive. Add planned rhythmic activities such as dancing, drumming, swinging, walking, and breathwork into the day to keep both children and adults regulated.
6. Respectful (of the child, family, and culture)
All trauma-sensitive interactions must be based on a deep respect for the child, family, and culture. Perry writes, "Marginalization is a fundamental trauma."[8] Dismissing or invalidating the experiences of an individual or group creates dysregulation and a lack of safety. Environments that foster respect for the whole child promote growth, healing, and resilience.
Tips for respectful developmental interactions:
- Remember that children’s emotions are real and valid. It’s easy to dismiss children’s feelings as silly or inconsequential, particularly if they are communicated in ways that feel irritating or over-the-top to adults. Relationships are strengthened when adults can co-regulate, actively listen, reflect the child’s thoughts and feelings, and communicate empathy.
- Be aware of the impact of race and culture on adopted children’s identities. Research indicates that raising transracially adopted children to be "colorblind" or ignore racial differences often causes them to feel “racially alienated with an unavoidable experience of racial stigma that was invalidated by parents."[9] Providing children with racial mirrors, initiating conversations about race, and learning from adult transracial adoptees is crucial for adoptive parents.
I spend far more time making dinner and driving kids to school than I do studying the inner workings of the human body, yet over the past decade I’ve watched my son’s brain grow. I’ve seen his sensitized stress response system become less reactive and more responsive through rhythmic, repetitive activities. I’ve watched his attachments grow as his relationships increased, both in number and in quality, and I’ve seen our family and this amazing boy make the leap from surviving to thriving. I’m a mom, not a neuroscientist, but the Neurosequential Model allows me to think like one, to meet my kids where they are, and to celebrate them as they heal and grow.
Further Resources to Explore
About the Author
Allison Cooke Douglas, M.S. is the Resource Center Program Manager at Harmony Family Center in Knoxville, TN. She has been teaching for over two decades; starting her career as a Montessori trained early childhood educator. After seeing a need for robust, trauma informed education for foster families, Allison become the lead Parents as Tender Healers (PATH) training specialist in Knox County, TN facilitating classes for prospective foster parents. She has held a variety of positions in state and regional Foster and Adoption Care Advocacy groups, served as a team member on a Breakthrough Series Collaborative project focusing on trauma assessment and treatment for children under 4 and is a trainer for Tennessee’s Building Strong Brains: ACEs Initiative. Allison is certified in Phases I and II of The Neurosequential Model of Therapeutics, as well as in the Neurosequential Model in Education. She is currently a fellow in the Napa Infant-Parent & Early Childhood Mental Health Fellowship at U.C. Davis. She and her husband Jonathan are grateful to share their lives with their four children, adopted via foster care.

Learn more about Allison at:
Harmony Family Center
References
[1] Perry, B. D., & Ludy-Dobson, C. R. (2010). The Role of Healthy Relational Interactions in Buffering the Impact of Childhood Trauma. In E. Gil, Working with Children to Heal Interpersonal Trauma: The Power of Play (pp. 26-43). Guilford Press.
[2] Hambrick, E. P., Perry, B. D., & Brawner, T. W. (2019). Timing of Early-Life Stress and the Development of Brain-Related Capacities. Frontiers in Behavioral Neuroscience. doi:10.3389/fnbeh.2019.00183
[3] Neurosequential Network. (2020, March 30). 3. Emotional Contagion: Neurosequential Network Stress & Trauma Series. Retrieved from YouTube: https://www.youtube.com/watch?v=96evhMPcY2Y
[4] Purvis, K. B., Cross, D. R., Dansereau , D. F., & Parris, S. R. (2013). Trust-Based Relational Intervention (TBRI): A Systemic Approach to Complex Developmental Trauma. Child & Youth Services, 360-386.
[5] Institute of Medicine and National Research Council. (2014). New Directions in Child Abuse and Neglect Research. Washington D.C.: The National Academies Press.
[6] Perry, B. D., & Winfrey, O. (2021). What Happened to You? Conversations on Trauma, Resilience, and Healing. New York: Flatiron Books.
[7] Rhythmic Mind. (2018, June 7). Dr. Bruce Perry Interview. Retrieved from YouTube: https://www.youtube.com/watch?v=a9NtmRj0tm8&t=12
[8] Perry, B. D., & Winfrey, O. (2021). What Happened to You? Conversations on Trauma, Resilience, and Healing. New York: Flatiron Books.
[9] Samuels, G. M., & LaRossa, R. (2009). Being Raised by White People: Navigating Racial Difference Among Adopted Multiracial Adults. Journal of Marriage and Family, 80-94.
Originally published in 2021 by National Council For Adoption. Reprinting or republishing without express written permission is prohibited.



